
The ART Model
The ART model essentially provides a framework for recovery oriented mental health care in a setting where people receive intensive psychiatric treatment. The ART model has been developed in close cooperation between the partners in the triad (service users, resource group and professionals). Several stakeholders and experts of 20 Dutch organizations collaborated in order to establish a new nationwide framework in long-term mental health care.
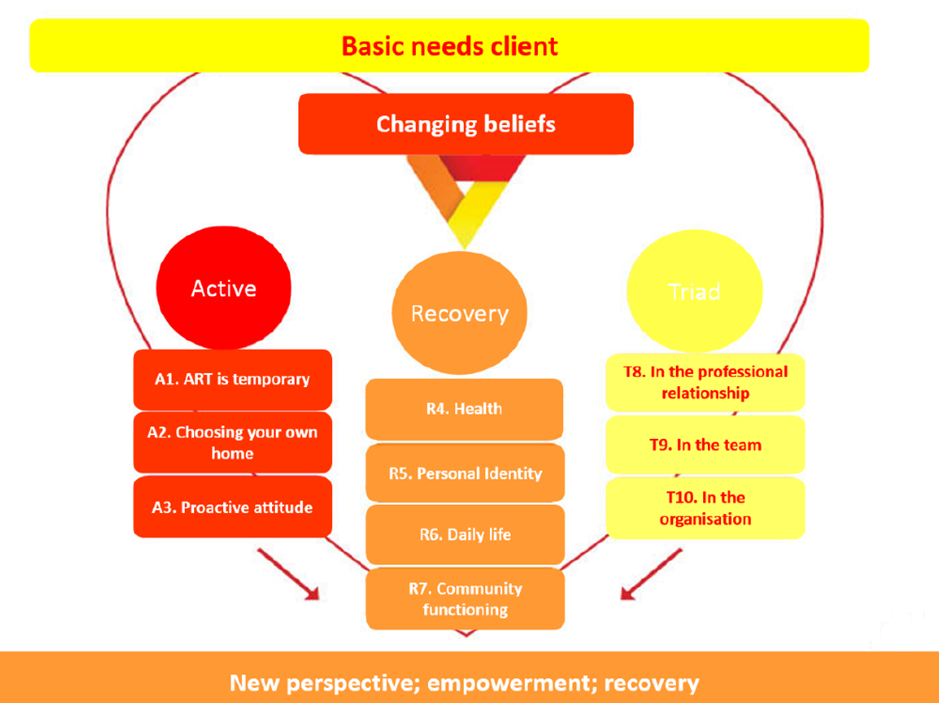
The basic human needs of the service users are the starting point and main focus of all the support and care people receive (basic needs client). But of course, the mental health care does not exist in a vacuum, there are changing beliefs and changing policies that influence the content and organization of the mental health care (changing beliefs). The acronym of ART contains the key pillars of the ART model: Active, Recovery and Triad.
Active
In order to improve recovery, an active attitude is crucial. The pillar ‘Active’ entails three components. First, ART is temporary (A1): ART-care has a maximum duration of three years. From the day of admission, it is examined what is needed to achieve this goal of three years. This delimited timeframe provides hope and a future perspective for service users and their resource group. In addition, it emphasizes the cooperation with outpatient care teams.
After three years, the ART care is evaluated with service users and their resource group on the basis of specific goals. Should three years be insufficient, the duration of ART may be prolonged with another three years. However, in that case external consultation is recommended to prevent continuing an unsuccessful treatment plan. Second, service users can choose their own home (A2). The principle of ‘housing first’ is leading; the first priority is seeking for a suitable accommodation. A safe place to live that meets the individuals needs is an important prerequisite for the recovery process, preferably in the community.
The third component is a proactive attitude (A3) for service users, family and mental health workers. For example, service users should be aware that taking (well-considered) risks are important in the recovery process. For mental health workers a positive and proactive attitude, embracing the “presence-theory” is essential in supporting service users in their recovery process. This implies working according along the principles of recovery oriented care. Finally, a proactive attitude of the family is important to support the service user in reconnecting with the society. However, most service users in long-term mental health care have a small social network and little family contacts, together referred to as the “resource group”. Therefore, one of the aims in the ART model is to strengthen these contacts and cooperate with the resource group.
Recovery
The second pillar in the ART model is ‘Recovery’. For service users of long-term facilities the concept ‘recovery’ is often unknown (associated with full recovery) or perceived as not feasible. Therefore, it is important to introduce this concept properly and empower service users to believe in their ability to recover. This pillar entails four intertwined levels of recovery: recovery of (mental) health, personal identity, daily life and community functioning.
First, recovery of (mental) health (R4) is associated with recovery of psychological and physical health. The ART model states that people have the right to not only obtain good psychiatric care but also good somatic care. It is important to examine the situation of every person individually, instead of providing only the necessary mental health care based on a diagnosis. Because of the connectedness between physical, psychological and social well-being, the cooperation between mental health workers, the GP, the dentist and other health workers is important.
Second, recovery of personal identity (R5) aims at a holistic approach rather than only focus on mental health aspects. The personal story of the service user is important in order to place events into context.
The third level of recovery is recovery of daily life (R6). The ART target population experiences severe problems in daily functioning. Stimulating service users to slowly perform daily activities again is important for the recovery process. Finally, recovery of community functioning (R7) refers to supporting service users in obtaining suitable and meaningful social roles. This may vary from payed labor to daily activities in a community setting.
Triad
The third pillar of the ART model is ‘Triad’, which refers to the triad of the mental health worker, the service user and the resource group. The triad should be present at the level of the therapeutic relationship (T8), at the level of the team (T9) and at the organizational level (T10).
Part of ART care is a more established role of the resource group in the recovery process of the service user (triad in the therapeutic relationship). The triad in the team involves the employment of client- and family experts by experience as part of the ART team. The knowledge and experiences of these two groups are beneficial for the provided care.
The triad in the organization (T10) refers to the importance of the perspectives of service users and recourse groups in policy making from the beginning of the process, and not solely upon finalizing a project or policy. It should be mentioned that within this framework, a person can have different roles. For example, a psychiatrist can also be part of a resource group in another situation, because his brother has a psychotic illness.
The ART model states that it is important to integrate these different roles in order to establish mutual relations and improve mental healthcare.
ART into practice
Translation of the ART model into practice is described in detail in the workbook ART, which contains suggestions with respect to changing the healthcare process according to the ART-model. This affects the whole healthcare process from admission (or sometimes sooner) and intake where the indication criteria of ART will be examined, to the interaction and first contact between the service user and organization of the care coordination meeting. Family and significant others should be involved and if these are minor or absent, the contact should be restored. The concept of recovery should be introduced and the needs, strengths and wishes of the service user and the resource group should be defined; this should be the basis of the integrated treatment plan.
The ART monitor
Similar to HIC, FHIC (Forensic HIC), and FACT, the ART model includes an instrument that enables the assessment of professional, organizational, and architectural characteristics of ART: the ART monitor. This monitor is developed in order to examine the quality and model fidelity of the care provided by an ART team. In addition, it provides a concrete framework that contributes to the implementation process of ART. The ART model, the validated HIC monitor, the FACT scale and scientific literature are the basis of the ART monitor. The monitor contains 54 items, divided into eight domains: team structure, team process, recovery oriented care and treatment, organization of care, professionalization, architectural design, safety and law context regarding coercion. The score on the ART monitor involves a 5-point Likert scale on all 54 items, ranging from ‘not verifiably implemented’ to ‘fully verifiably implemented’.